Field notes
-
Preface: Healthcare Is Compressed Coordination
Compressed Medicine · Preface · How to read the curriculum
Healthcare is compressed coordination under uncertainty. Clinical communication works when agents reconstruct sufficiently aligned belief states from minimal messages. Clinical safety fails when those compressed models silently diverge. Clinical AI should become the infrastructure that exposes, synchronizes, and corrects belief states before irreversible action. This curriculum walks that argument across eleven parts.
-
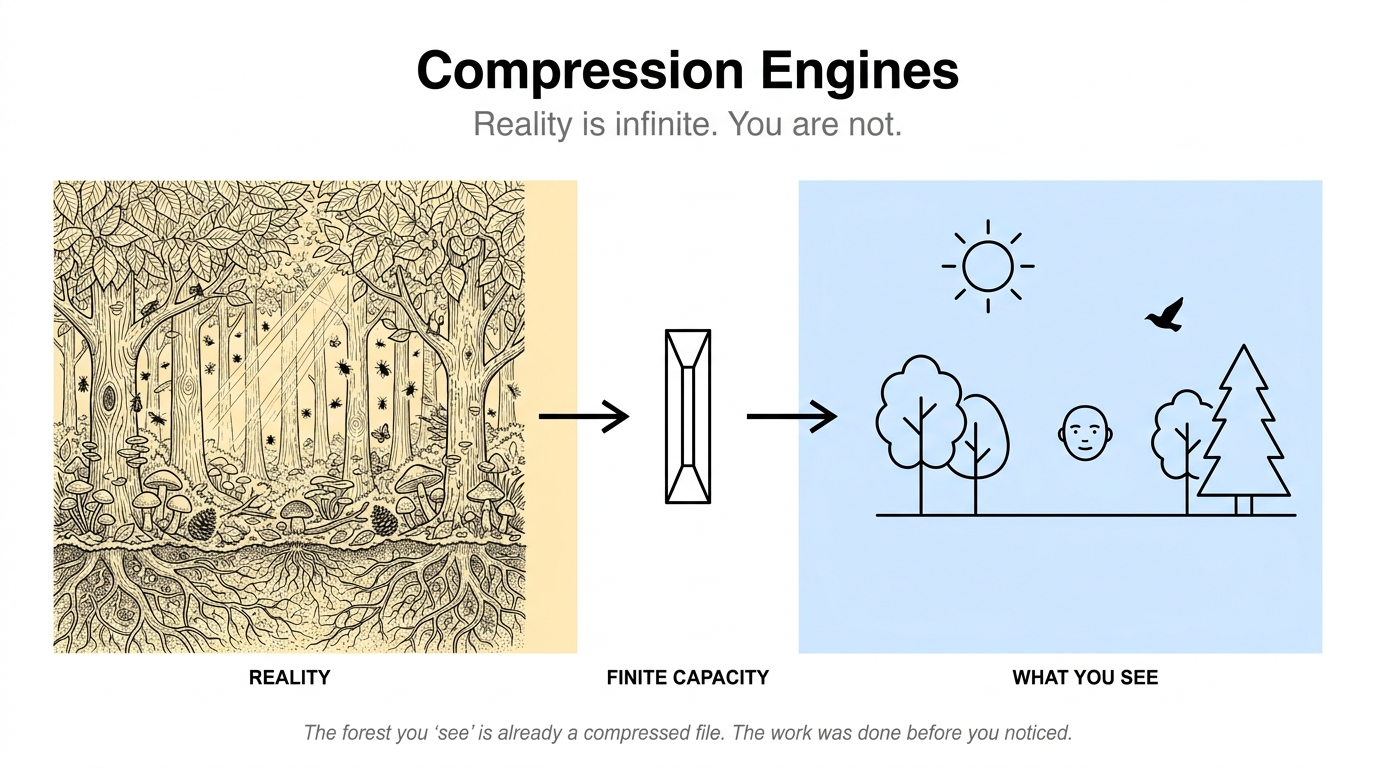
Compression Engines
Compressed Medicine · 1. The Compression Substrate · Why everything we see is already a compression
Reality has infinite detail. You have a few pounds of brain. The math does not work, which is why everything we do is a kind of compression.
-
The Function of the Message
Compressed Medicine · 2. The Function of the Message
Compression is utility-relative. The right clinical message depends on three things simultaneously: the function it must perform, the receiver who must decompress it, and the total cost the representation imposes. A handoff, a consult question, a discharge summary, a progress note, and a teaching point on rounds are five different compressions of the same patient. The best message is the lowest-cost sufficient representation for the receiver's objective and architecture.
-
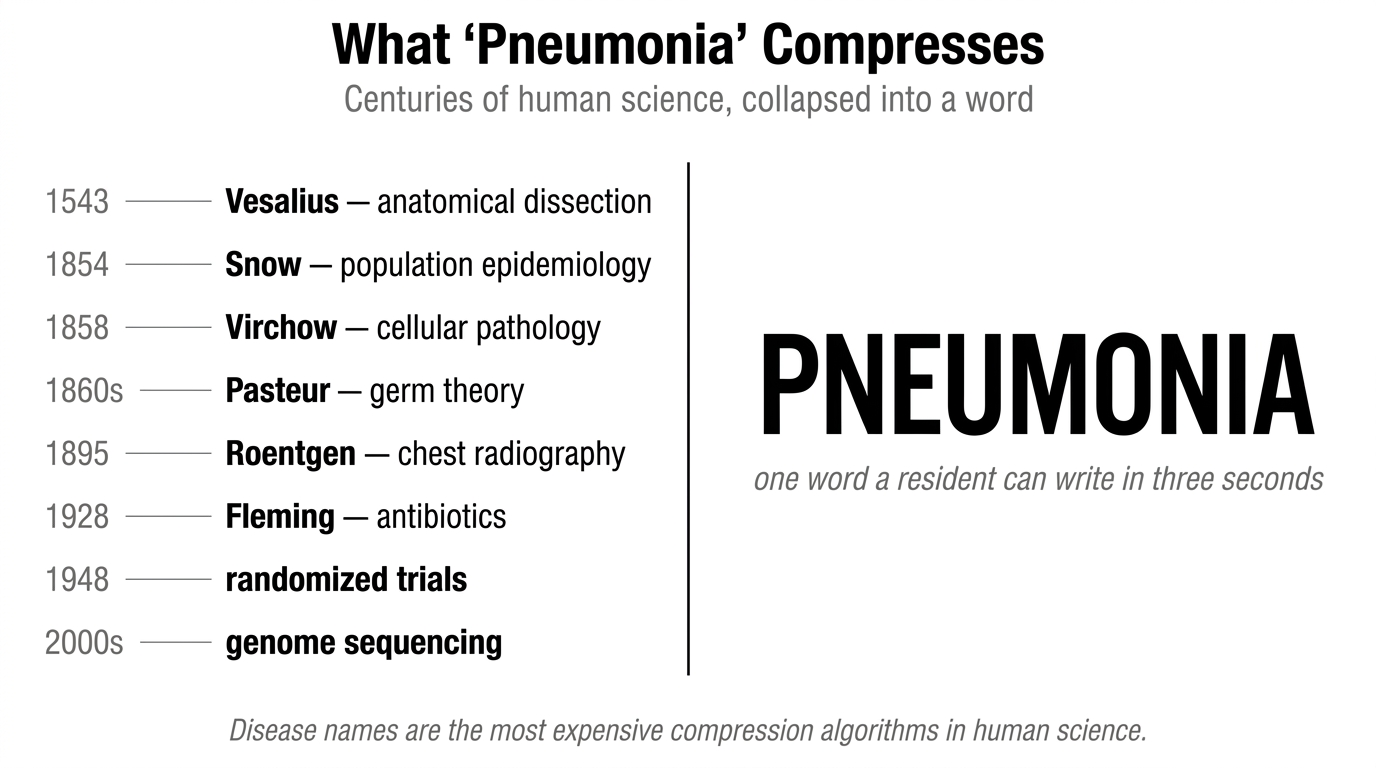
The Highest Accurate Abstraction
Compressed Medicine · 3. The Highest Accurate Abstraction
Clinical messages should compress to the highest level the receiver can accurately decompress. Handles point at patterns; richer patterns load more model per token, which is why the compression hierarchy exists at all. Accuracy means predictive fidelity: the predictions the message carries verify when checked. Clinical messages compress along four axes that are minimum-sufficient for action (state, trajectory, action, confidence), each receiver-relative through codec-gap. The operational rule: compress upward until prediction would break.
-
The Decompression Order
Compressed Medicine · 4. The Decompression Order
Once the abstraction level is chosen, the message should unfold in a predictable order: base model first, relevant nuance second, evidence and action third. The base model lets the receiver orient. The nuance prevents overgeneralization. The action tells them what changes management. The opposite order forces the receiver to back-build the model from evidence.
-
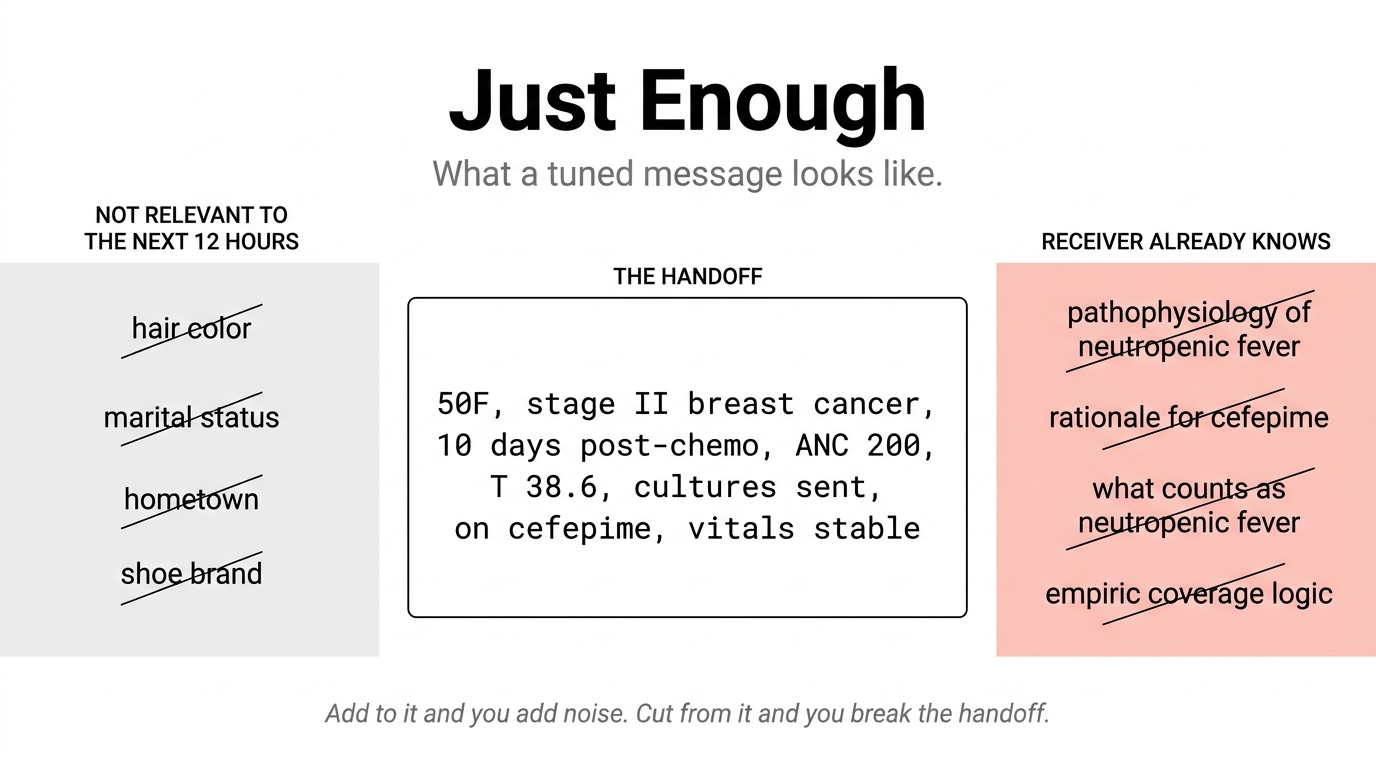
The Minimum Sufficient Message
Compressed Medicine · 5. The Minimum Sufficient Message · Just enough, the principle of the tuned message
What does it look like when a message has been tuned to a point? A physician's twelve-second handoff, and the principle behind it: every word still earning its place, nothing left in that the receiver could supply themself.
-
The Grounding Constraint
Compressed Medicine · 6. The Grounding Constraint
Compressed clinical claims need grounding, but not unlimited grounding. Include the evidence that would cause the receiver to reconstruct a different model if absent. Omit the rest. The goal is not maximal brevity; it is controlled decompression. The receiver should not merely hear the words. They should reconstruct the intended state.
-
The Belief-State Object
Compressed Medicine · 7. The Belief-State Object
Up to now the series has talked about how clinicians compress messages. This essay asks what is actually being compressed. The answer is not the chart, not the patient, and not a list of diagnoses. It is a structured belief state: a mixture distribution over hypothesis-components, each carrying its own evidence dependencies, predicted trajectory, action threshold, and disposition implication. The structured belief state is what training builds, what handoffs transmit, and what clinical AI has to maintain.
-

The Same Wall
Compressed Medicine · 8. The Same Wall · The substrate-independent failure mode
Agents act on compressed models, communicate through lossy channels, and mistake shared words for shared state. The same failure mode appears in clinical medicine, intelligence analysis, aviation, and distributed systems. Other fields installed partial structural mitigations. Clinical AI has the architecture of the unmitigated era.
-
The Defense Architecture
Compressed Medicine · 9. The Defense Architecture
Medicine defends against divergent compressed models through two operations: shared compression (training agents to encode reality similarly) and error correction (catching divergence when shared compression fails). Clinical AI should implement both. The product is not an answer generator. It is a belief-state coordination system that maintains shared compression across the team and runs error correction continuously.
-
The Temporal Loop
Compressed Medicine · 10. The Temporal Loop
Belief-state alignment is not a runtime-only operation. Medicine defends across three temporal layers: pre-event alignment through training and standardized scripts; runtime synchronization through handoffs, consults, and verification mechanisms; post-event update through outcomes, M&M, and calibration tracking. Clinical AI should implement all three, continuously, with each layer feeding the next.
-

The Connection
Compressed Medicine · 10.1 The Connection · Verification is observable signal meeting explicit state
Verification is observable signal meeting explicit state, at moments the architecture chooses to listen on. The clinician is a privileged channel into reality, but not the verification target. The architecture wires four signal channels into a single inspectable state object and chooses, per moment, whether to confirm, update, flag, or gate.
-

Quiet Verification
Compressed Medicine · 10.2 Quiet Verification · Passive by default, active for closure
Any verification mechanism that costs the clinician visible time at 3 a.m. will be bypassed, and bypassed often enough becomes bypassed reflexively. The verification architecture that survives this puts almost all of its work on channels the clinician does not have to spend attention on, and reserves a small, AI-targeted active read-back for the one gap no passive method can cover.
-
Quiet Acquisition
Compressed Medicine · 10.3 Quiet Acquisition · The other half of the closed loop
Quiet Verification covered the architecture for surfacing mismatches between signal and inference without spending clinician attention. There is a symmetric problem on the other side. The inferences the system holds are only as good as the signals that fed them, and the signals that did not arrive are invisible by definition. The closed-loop architecture also needs an acquisition layer that detects what has not been asked, has not been measured, has not been observed, and does it quietly.
-
The Irreversible-Action Check
Compressed Medicine · 11. The Irreversible-Action Check
The highest-value moment for clinical AI is immediately before irreversible action. Before discharge, escalation, sign-off, hand-off, or closing a workup, the architecture should expose, synchronize, and correct belief states across the team. The capstone of the curriculum: clinical AI is a belief-state coordination layer for healthcare, and the action moment is where that coordination matters most.
-
The Process of Doctoring
Companion to Compressed Medicine · You treat the patient, not the label; the diagnosis is one handle in your model of her
A patient's actual state, the real pathology and physiology and trajectory in the body, is hidden; the clinician sees only partial signals and builds a working model from them. Early on, the honest form of that model is not one diagnosis but a ranked set of live possibilities, weighed for plausibility and danger: a differential. The diagnosis is one handle inside the model; the patient-specific details the label leaves out are usually where the action lives. You manage the actual patient, through the model, by gathering only the information that could change what you do and updating whenever her response comes back. This essay walks one breathless patient through the loop. A clinical companion to the Compressed Medicine series.
-
Why Your Retrieval Stack Never Converges
Companion to Compressed Coordination · Semantic match is task-relative, not absolute
Vector search misses. You add BM25, you stack a reranker, you fine-tune embeddings. Each layer catches what the last missed and misses what the last caught — and many developers hitting that wall are stacking solutions to a problem that was not a retrieval problem in the first place. This essay's most practical move is upstream: a triage that tells you whether retrieval is the operation your task actually needs, and whether top-k similarity can reach the answer even when it is. For the cases that pass triage, the conceptual shift follows: there is no task-free semantic match for the stack to converge on; there is only the task-sufficient match that exists relative to the downstream decision. Translates the equivalence-class result of Compressed Coordination into the vocabulary and symptoms of retrieval engineering.
-
Compressed Coordination
Companion to Compressed Medicine · The general theory the clinical curriculum instantiates
Bounded agents communicate through lossy signals that underdetermine the source state; receivers must reconstruct using priors and context. Coordination succeeds not by recovering full meaning but by preserving the distinctions that change action — though which distinctions matter depends on whose utility function defines the partition. The clinical curriculum's three failure modes (asymmetric updating, silent reconstruction, shared-vocabulary divergence) become expressible within this framework rather than asserted from outside it; a fourth — strategic underdetermination — is the framework's most original move and emerges when sender and receiver have misaligned utilities. Multi-modal AI, AI-to-AI coordination, distributed systems, biology, and science instantiate the same architecture in different substrates. The bounded-resources axis this essay develops is one of several; the broader multi-axis framework is the territory of the companion essay.
-
What Determines Whether Coordination Survives
Companion to Compressed Coordination · The full multi-axis framework
Six axes determine whether bounded agents can coordinate: resource bounds, learning history, substrate heterogeneity, channel properties, incentive structure, and system-level structure. Each produces distinct failure pressure independently. The framework is testable to the extent each axis has a distinguishable sensitivity profile on measurable observables — coordination failure is a surface in axis-space, not a single dimension. Four predictions follow: recursive codec drift between adapting agents, axis-specific intervention sensitivities, strategic underdetermination scaling with verification cost, and multi-agent system-level failures that don't reduce to individual capacity. Each is testable; each has a stated falsifier.
-
A Third Processor
Absorbed into the Compressed Medicine curriculum
This essay was an early draft. Its argument — that a clinical AI is another codec in the chain, not just a smarter wire — has been absorbed into Parts 1, 2, and 8 of the Compressed Medicine curriculum. The Mayo ambient-scribe case it documented is in Part 8.
-
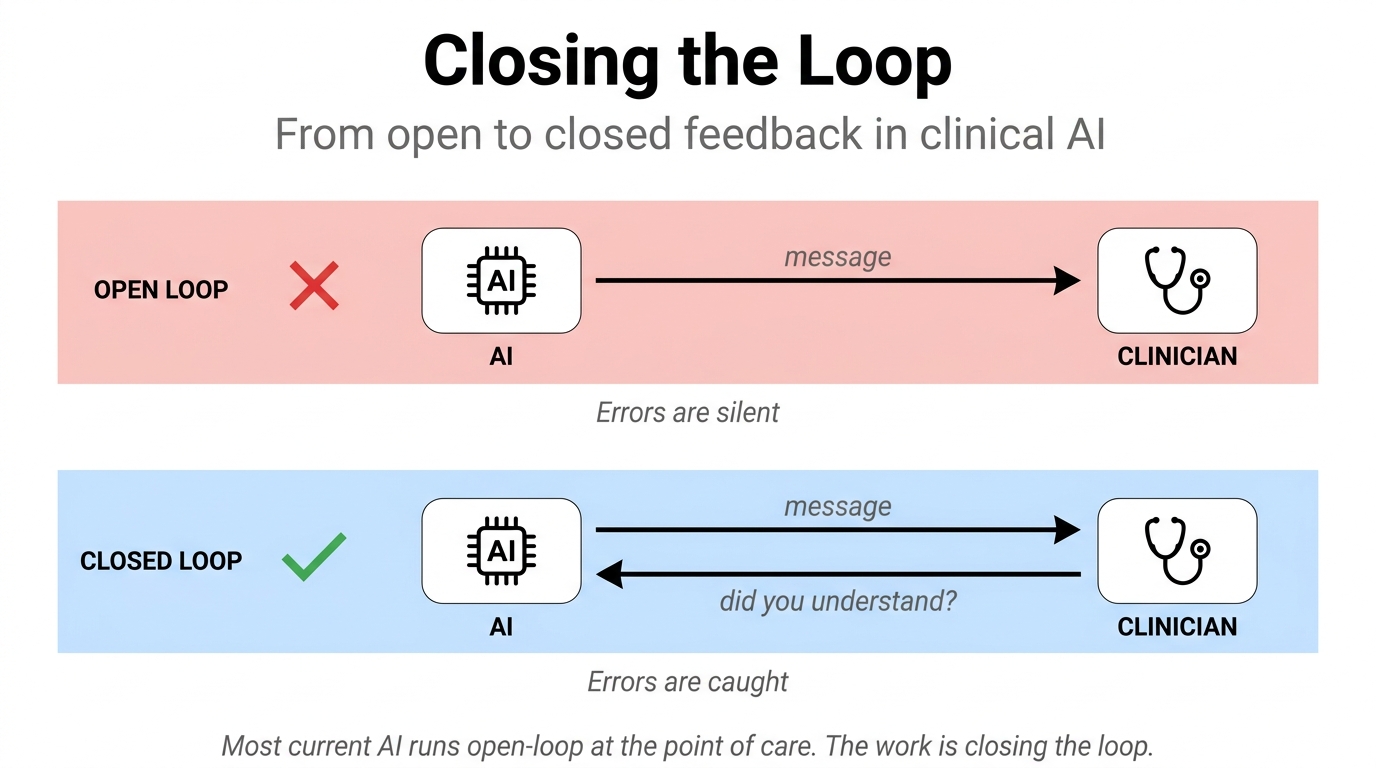
Closing the Loop
Absorbed into the Compressed Medicine curriculum
This essay was an early draft. Its argument has been absorbed into the Compressed Medicine curriculum — primarily into the Defense Architecture (Part 9), with specific cases folded into Parts 8 and 11.
-
Coda: The Closed-Loop Checklist
Absorbed into the Compressed Medicine curriculum
This essay was the v1 synthesis of a six-essay argument. Its substance has been absorbed into the Compressed Medicine curriculum — the architecture argument into Part 9, the production-failure citation into Part 9, and the framework-comparison positioning into the Preface.
-
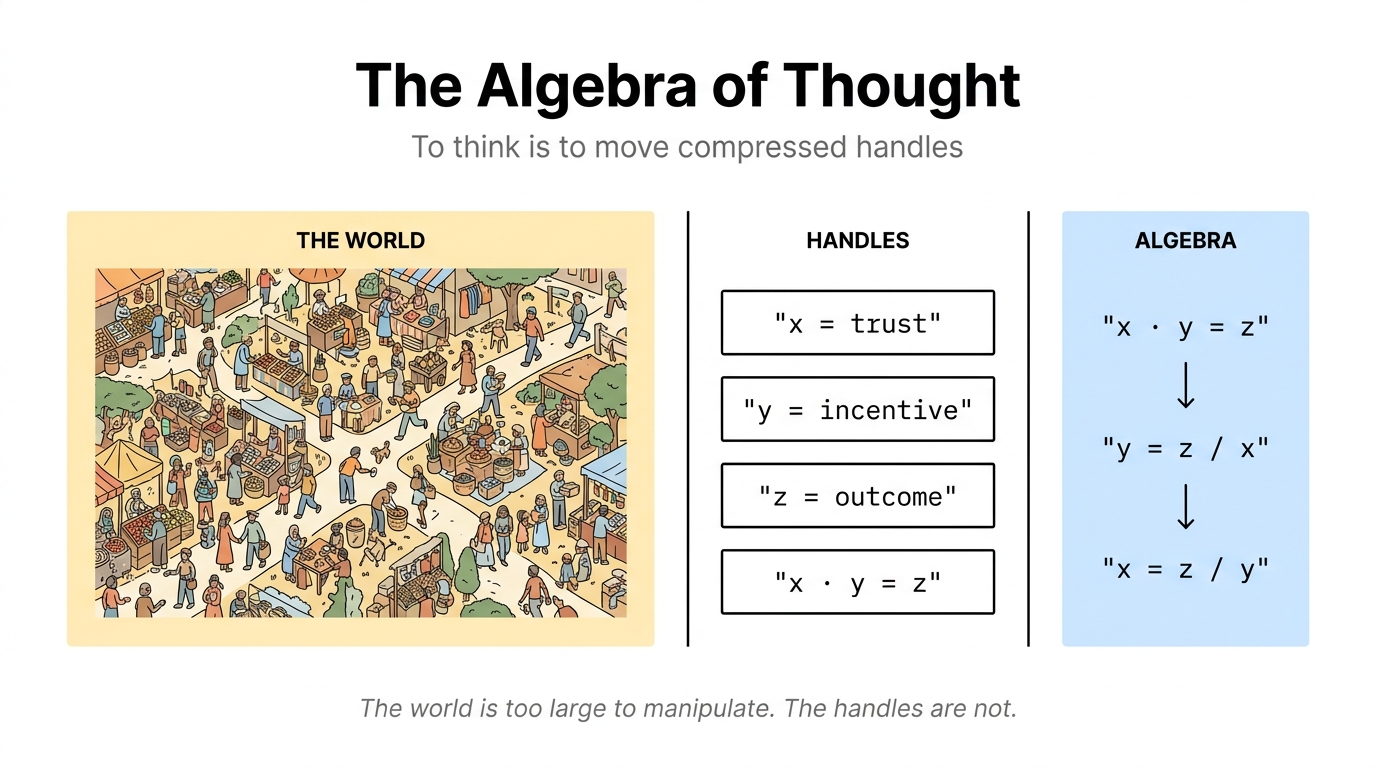
The Algebra of Thought
Companion to Compressed Medicine · To think is to compress and decompress
To think is to compress and decompress. Algebra is thought made visible; everything else we call thinking is the same operation in less obvious form. Finite minds cannot do anything else.
-
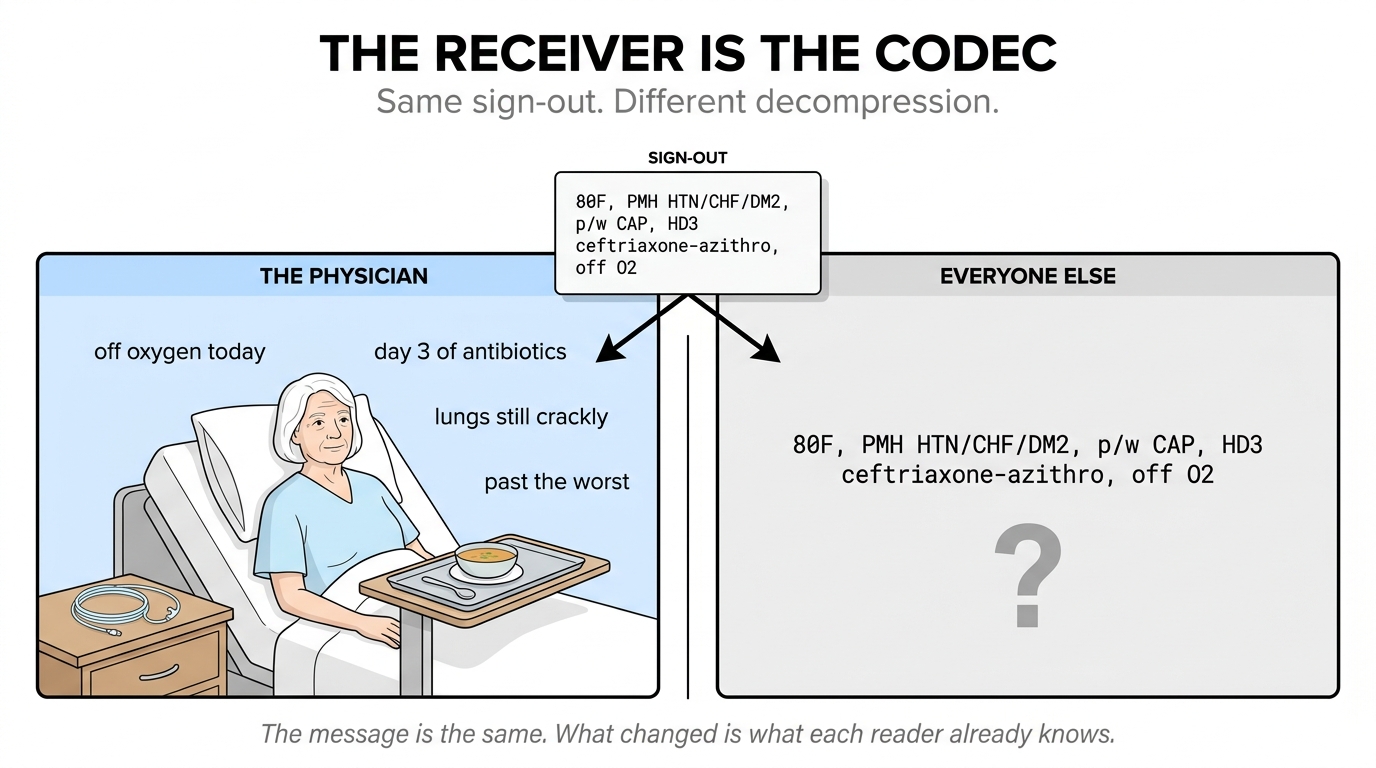
The Receiver Is the Codec
Companion to Compressed Medicine · Communication as a property of the receiver
The same line of shorthand can be brilliance to one person and noise to another. Efficient communication is a property of the receiver, not the sentence.
-
Clinical AI's Binding Problem
Diagnosis is compression. Care is binding. The unsolved problem in clinical AI isn't enlarging the cache; it's binding the cache to the specific person in front of you.
-
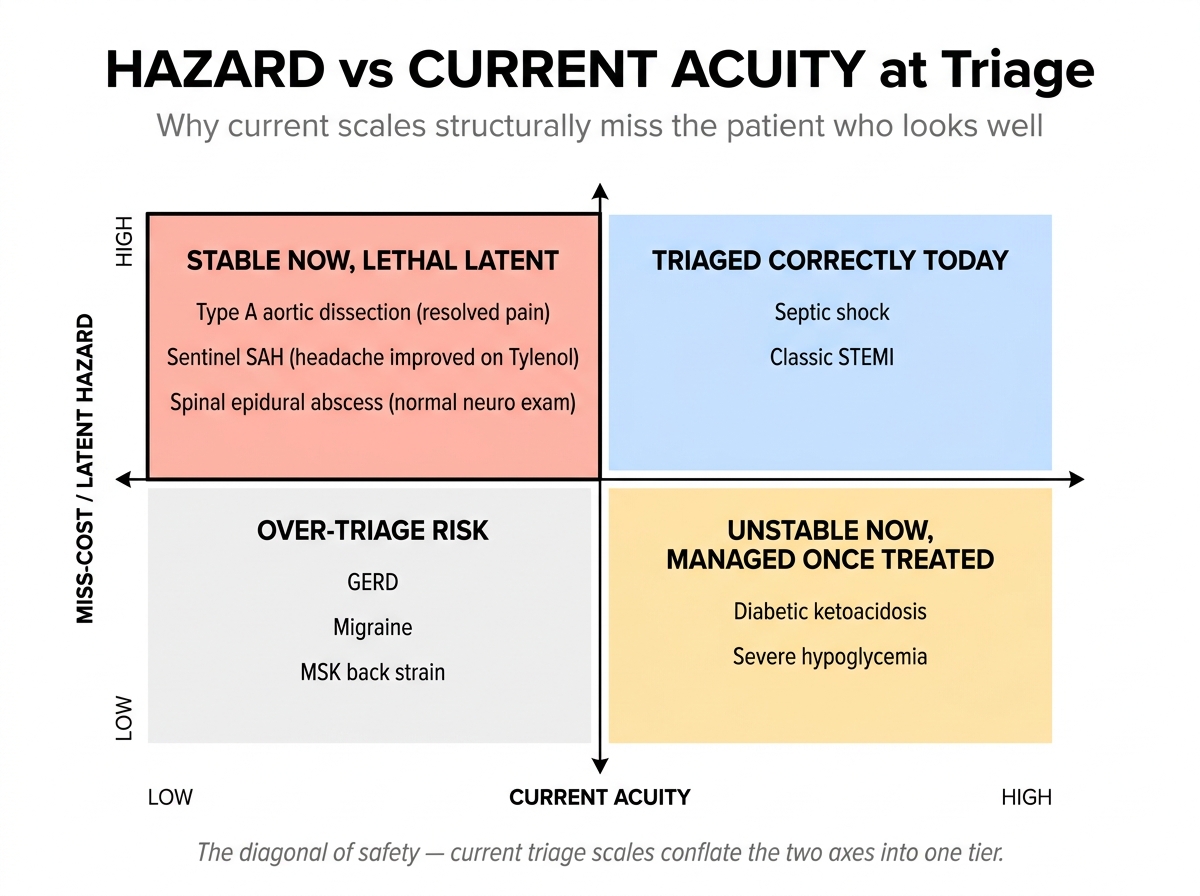
The Minimum-Information Problem: Why Triage Is So Hard
Triage is risk allocation under irreducible uncertainty, not diagnosis. Three worked clinical examples show why the seasoned clinician's eye, paired with structured candidate-with-hazard reasoning, is the foreseeable best architecture.