The Process of Doctoring
Companion to Compressed Medicine · You treat the patient, not the label; the diagnosis is one handle in your model of her
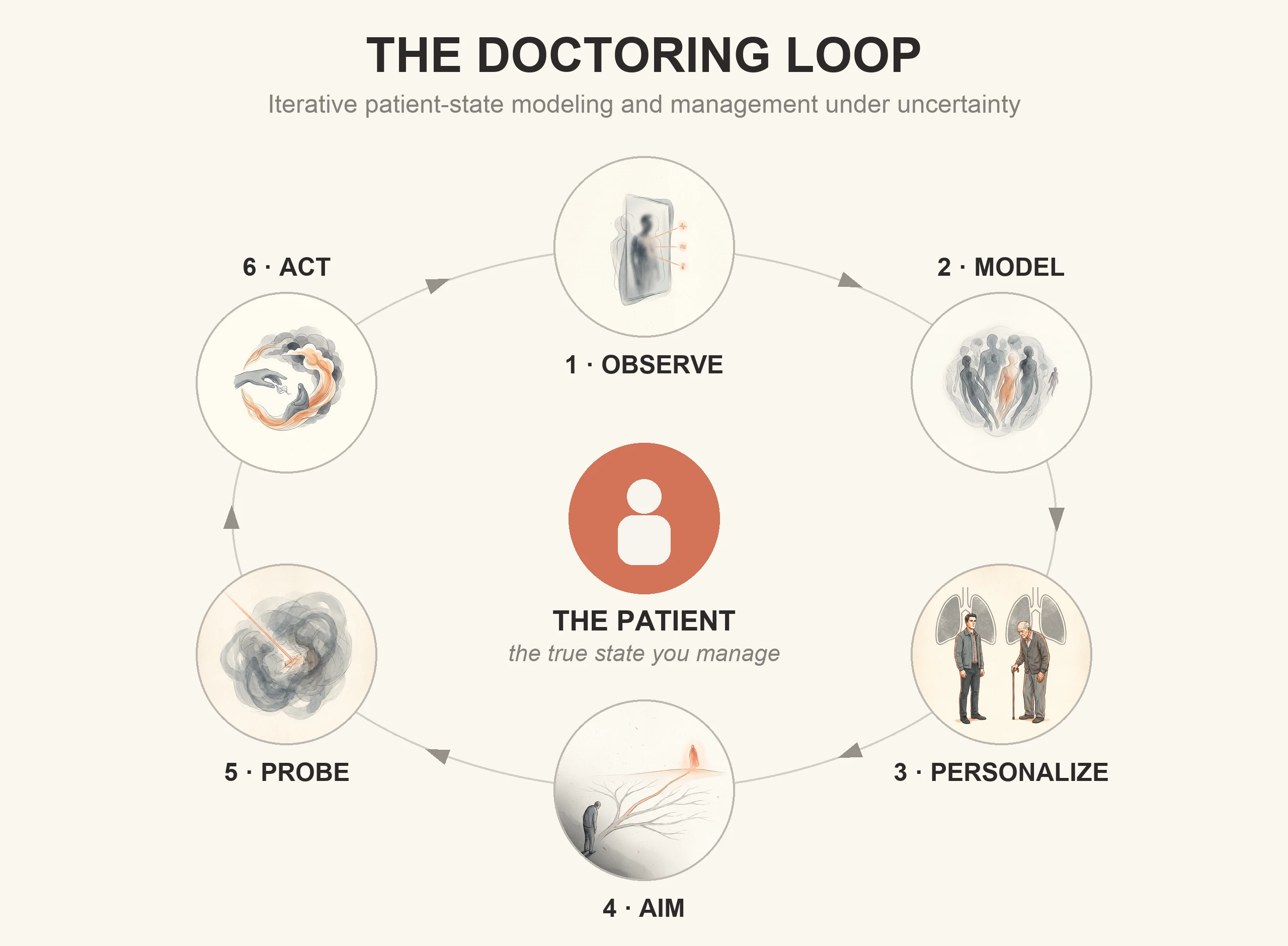
From the outside, doctoring looks like reaching a diagnosis. The diagnosis matters, but it is not what you are managing. The patient is. Every patient has an actual state: the real pathology, physiology, and trajectory in the body, which you can never see directly, only infer from partial signals. What you build from those signals is a working model of it, and you treat the patient through that model. The work is a loop: build the model, reduce the uncertainty that matters, act, and let the response correct it. These steps are easier to separate on paper than at the bedside, where they overlap and, in a crashing patient, blur into seconds. What follows walks one patient through the loop.
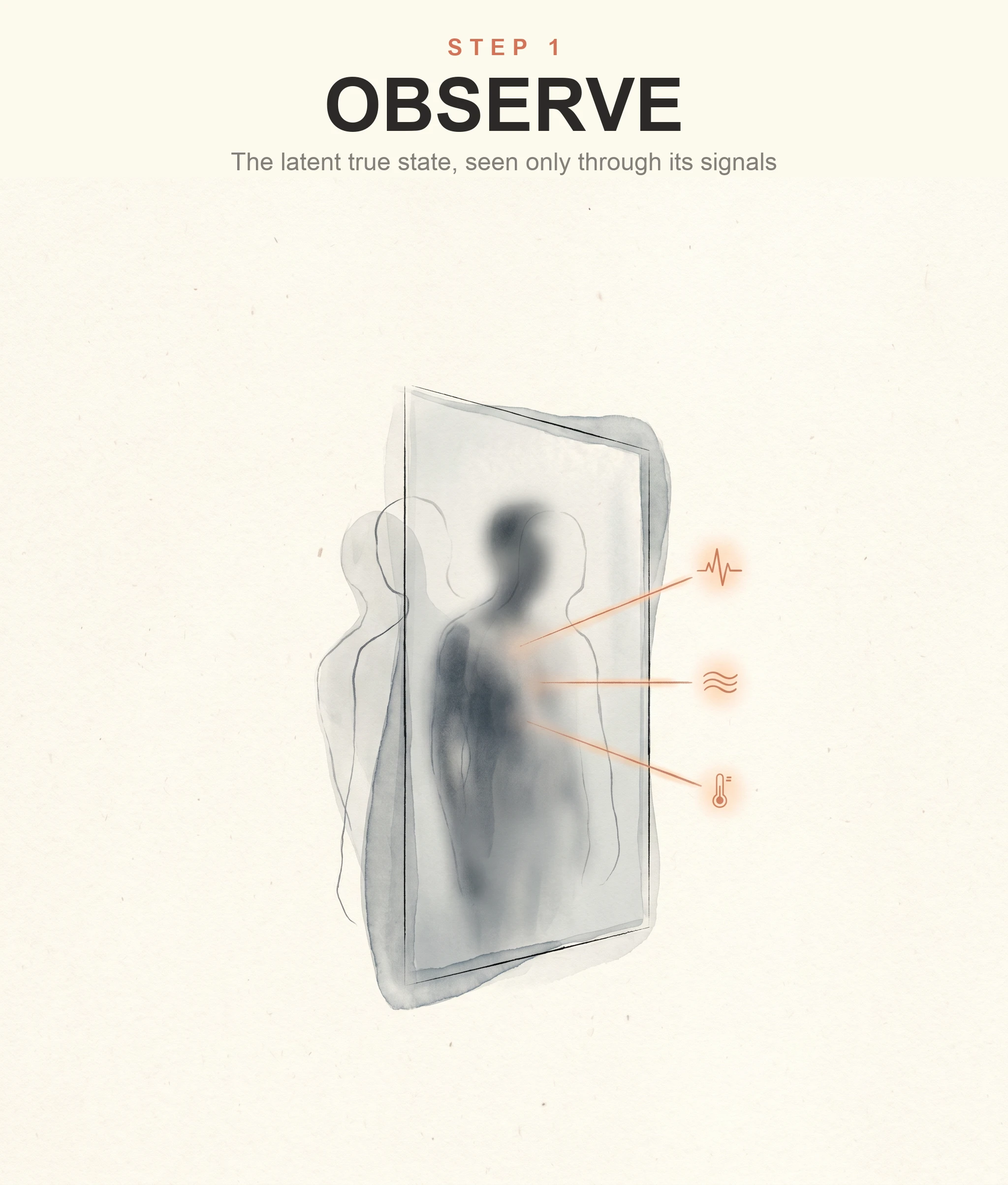
1 · Observe
A woman in her late seventies arrives short of breath. At first that is almost all you have: she is breathing fast, she looks frightened, her oxygen is low, she has a fever, and her blood pressure is on the soft side. Behind those few facts is one real state, but you cannot see it directly. You see the shadow it throws. Pneumonia throws that shadow. So does heart failure, a pulmonary embolism, a COPD flare, sepsis, or two of them at once. The same presentation underdetermines the diagnosis: many states fit the handful of signals in front of you. She has one state. Your access to it is partial. Doctoring begins in that gap.
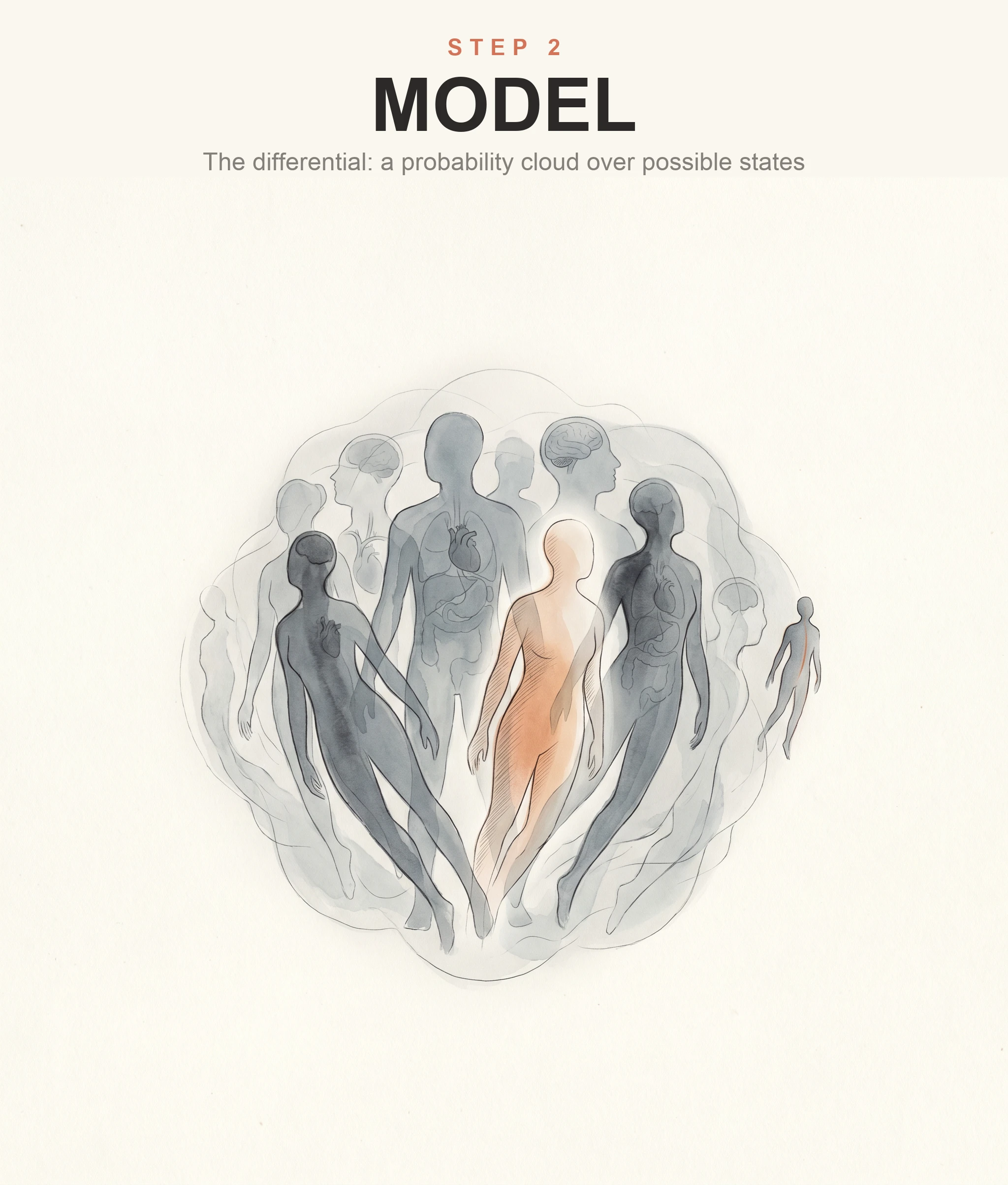
2 · Model
Because her state is hidden, you usually cannot honestly collapse the case to one diagnosis yet. Naming a single answer too early invents certainty you don't have. What you build instead is a working model, and early on its honest form is a distribution: a ranked set of live possibilities, each weighed for how plausible it is and how dangerous it would be to miss. That is what a differential diagnosis is at its best. Not a list to cross off one by one, but your current sense of what may be happening, a cloud of possibilities that is denser where the evidence points. Pneumonia, likely. Heart failure, plausible. A pulmonary embolism, less likely but dangerous. Hold that spread without freezing, and act inside it rather than wait for it to collapse to one answer.
3 · Personalize
Each possibility is a generic model. "Pneumonia" is what is common to everyone who has it: the expected findings, the usual course, the standard treatment. That is its power and its limit. A label, by construction, is what cases share; to be a label at all it must leave out whatever makes one case differ from another.
What it leaves out is most of the patient. For this woman: her kidneys are failing, she is frail, she is already on home oxygen, she lives alone, and she has told you before that she never wants to be intubated again. None of that is in the word "pneumonia." These are the fine strokes, not decorative detail but the specifics the label does not carry, and usually the things that decide what you do. The same "pneumonia" in a healthy thirty-year-old would be a different patient entirely.
So your working model is not the generic disease. It is that set of hypotheses conditioned on this person: her physiology, her limits, her goals. The conditioning is what decides the action.
4 · Aim
The diagnosis is a handle, not the object. What you are moving is her actual state, and the target is the best outcome still reachable for her from here. The target is not fixed at "normal"; it is whatever future is still reachable given her biology, the time you have, the resources at hand, and what she wants. And it is not one thing, or one at a time. At any moment you are holding several at once, layered. The large one is the destination: treat what is treatable without a tube, and keep her comfortable and clear-headed enough to be with her daughter. Beneath it sit the immediate ones: get her oxygen up, hold her pressure. Running alongside both, not before them, is a question you still need answered, whether her lungs are wet or infected, because it changes how you pursue the rest. The big goal frames the small ones, and the small ones are how you move toward it. None is fixed: as she responds, any of them can shift. The goal is a variable, not a constant, and the aim updates with evidence, just as the model does.
5 · Probe
Between where she is and where you want her sits information, and not all of it is worth having. A question, an exam, a test, a stretch of watching earns its place when it could change something you do: the treatment, how closely you watch her, where she goes next, what you tell her and her daughter. A bedside check: if this came back the other way, would I do anything differently? If not, be honest about why you are ordering it. For her, an ultrasound that separates fluid-filled lungs from pneumonia is worth more than a test whose result you would treat the same either way.
6 · Act
You act when the model is good enough to justify the move, or when waiting has become more dangerous than acting, which in medicine is often, because certainty is usually unavailable, unnecessary, or too slow to be safe. But notice that the probe already changed things. When the ultrasound shows wet lungs, the model shifts toward heart failure before you have given a single drug. Every move you make, to learn or to treat, sends a signal back. The oxygen that climbs after diuresis. The pressure that does not budge after fluids. The patient who looks worse an hour after a plausible plan. Each is the world answering. You compare what the model predicted against what she actually did, and where they diverge, it is the model that is wrong, not the patient. The response is your next observation: you take it in, the model updates, and you go again with a sharper picture, a narrower aim, the next move. Probe and act are both moves, and both feed the update. That is what makes it a loop, not a one-time classification.
The same loop, run well
Novice and expert run the same loop. What separates them is how well each turn is done. The expert holds a wider range of possibilities, so the true answer is more often somewhere in the model at all, and a possibility that never enters the model can never be reasoned toward. The expert weighs them by plausibility and by danger both, keeping a low-odds catastrophe in view because missing it is unaffordable. The expert sees disease as a process in time, not a snapshot, and asks what the next hour should look like if the model is right. The expert reaches for the signal most likely to change the plan, not every signal available. And the expert keeps a wider set of moves: stabilize, temporize, monitor, escalate, refer, watch and wait. No one can choose a move they don't know exists.
What doctoring is
Strip it down, and doctoring is building and revising a model good enough to guide action, then using it to move the patient toward the best outcome still reachable. Her actual state stays hidden; the differential is your honest first sketch of it; the patient-specific details are what fit it to her; you gather only the information that would change what you do; you act; and her response rewrites the model. The loop runs until she reaches the best state still within reach, until her care passes safely to someone else, or until no further action would help.
The disease is not the object. The patient is. The diagnosis is not the answer; it is the model's most useful handle, the thing that lets you act before the truth is fully in.
This is the clinical version of ideas the rest of this series develops more formally. Medicine just makes them concrete, because the consequences land on a real person.