The Defense Architecture
Compressed Medicine · 9. The Defense Architecture
A cardiology fellow signs out an inpatient to the night hospitalist. "Mr. F, post-PCI to LAD this afternoon, on aspirin and ticagrelor, NPO until midnight then advance, telemetry, call for chest pain or new arrhythmia." Twenty-three words. The hospitalist nods, asks one clarifying question about heparin status, and accepts the patient.
Twenty-three words. The hospitalist did not need to be told what PCI is, what aspirin and ticagrelor do, why NPO before procedure clearance matters, why telemetry is standard post-cath, or what counts as a callable arrhythmia. The shared compression between the two clinicians did all of that work invisibly. They were trained on the same codec. The handoff worked.
The same twenty-three words spoken to a patient's son in the waiting room would not have worked. They would not have worked spoken to a hospitalist three years out of residency who never worked a cardiology service. They would not have worked spoken to a clinical AI scribe trained on outpatient text. The receivers there do not share the codec. The same compression that succeeds between the fellow and the night hospitalist fails everywhere the codec is not shared.
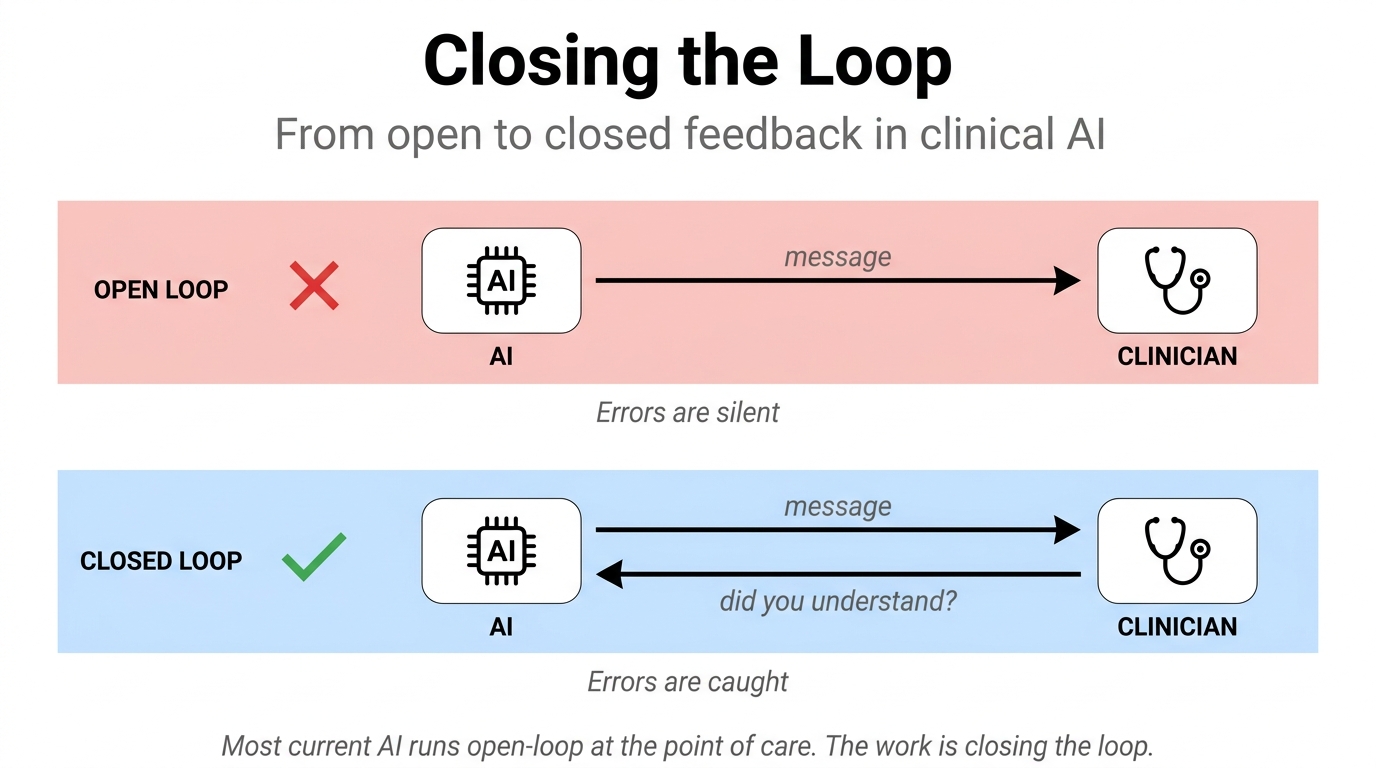
Medicine has been solving this problem for a hundred years. The defense architecture is two operations. Shared compression makes the receivers be able to decode the same messages the same way. Error correction catches when, despite shared compression, the decoded models have drifted apart.
The principle
Clinical AI should implement shared compression and error correction.
Not as a slogan: as the architecture. Clinical AI's product is a system that maintains shared compression across the team's agents (clinicians, consultants, nurses, AI, patient, family) and runs error correction continuously against divergence between those agents' belief states. Answer generation, summarization, and drafting are useful tools the system happens to expose; they are not its central function.
This is the synthesis principle the rest of the series builds toward. Parts 1-6 established the substrate; Part 7 named what is being compressed (the structured belief state). Part 8 established the failure mode (silent divergence between compressed models). Part 9 names the master defense: two operations, shared compression and error correction, applied together. Parts 10 and 11 will operationalize this across temporal layers (pre-event, runtime, post-event) and at the irreversible-action moment.
Shared compression: the first defense
Medicine already implements shared compression at scale. Medical school teaches a vocabulary: diseases, syndromes, signs, symptoms, drugs, procedures. Residency teaches a deeper layer: when each compression applies, what each one activates in the receiver, what discriminates between candidates, what action thresholds attach to each diagnosis. Attending feedback, illness scripts, guidelines, standardized order sets, professional culture: all of this is shared-compression infrastructure. By the time a new attending starts an unsupervised shift, ten thousand hours of shared compression has been installed.
Clinical AI extends this infrastructure to the AI side of the team. The system that helps the cardiology fellow and the night hospitalist communicate is not the system that emits English summaries. It is the system that maintains:
- Structured problem representation. Each active problem is a hypothesis-component with the eight fields Part 7 named.
- Standardized clinical state tokens. "Post-PCI day 0," "decompensated HF on diuresis," "low-risk chest pain by HEART score" function as model loaders the way Part 3's abstraction hierarchy described.
- Illness-script framing. Each active diagnosis carries the expected trajectory and the discriminating features that would unseat it.
- Consistent DDx structure across team members. The fellow's structured DDx, the hospitalist's, and the AI's are all instances of the same data structure, comparable for divergence.
- Explicit action thresholds. Each component carries the threshold at which workup or treatment commits.
- Shared risk language. "Low risk" means a numeric band, not a feeling. (Sherman Kent's words-of-estimative-probability fix from 1964 applied to clinical reasoning.)
- Evidence-linked claims. Each assertion in the chart, the dashboard, or the handoff carries a pointer to the evidence supporting it.
- Dashboard-level state representation. The shared compression is visible, inspectable, and constantly available to anyone joining the team mid-case.
These eight items are surfaces of a single system whose job is to make the team's compressions share the same codec, not eight separate features. Shared compression is the receiver-architecture alignment work named in Part 2 applied across the whole team: bringing each agent's representations close enough to each other that compressions emitted by any one of them decompress correctly in the heads of the others. Without that alignment, every cross-agent message has to do its own translation work from scratch, and the friction budget runs out. Existing AI techniques touch pieces of this work — retrieval-augmented generation (Lewis et al., 2020) implements external memory the model can reach at inference time, which is one mechanism for an externalized shared codec — but no shipped product treats shared compression across the human-AI team as the integrated infrastructure problem it is.
Error correction: the second defense
Shared compression is necessary and insufficient. Even when the codec is aligned, agents' belief states drift. A team that was synchronized at sign-out can be silently out of alignment by morning rounds. The structured belief state of the day team and the structured belief state of the night team can have diverged on the trajectory field, the action threshold field, or the disposition implication field, with neither team noticing until the divergence has consequences.
Error correction is the operation of detecting and repairing those divergences. Medicine already does this, partially: handoff questions, consult discussions, read-backs, predictions, repeat exams, follow-up labs, radiology overreads, M&M conferences, bounceback reviews, outcome feedback, debriefs. Each is an error-correction mechanism that takes some kind of divergence (between minds, between assessments, between expected and observed) and either confirms alignment or surfaces the gap.
Clinical AI is positioned to do error correction more continuously than humans can. The system can flag:
- Unsupported claims. The chart asserts "PE ruled out" with no test that would have ruled out PE.
- Stale assessments. The assessment from morning rounds is still the active belief state when the trajectory has changed.
- Plan-belief mismatch. The plan reflects an assessment the active evidence no longer supports.
- Unresolved dangerous diagnoses. A high-cost-of-miss hypothesis sits on the differential with no plan to exclude it.
- Missing key evidence. A hypothesis-component's action threshold is crossed but the discriminating test has not been ordered.
- Contradictory evidence. New signal contradicts the leading hypothesis without anyone surfacing it.
- Changing trajectory. The observed trajectory has diverged from what the leading component predicted.
- Clinician-AI disagreement. The clinician's actions imply a structured belief state that differs from the AI's.
- Disposition-risk mismatch. The discharge plan does not match the risk profile of the residual unexcluded diagnoses.
These nine items are classes of divergence the system watches for, surfaces only when they cross the action-relevance threshold, and surfaces in the friction-engineered way the Quiet Verification companion described. They are not nine separate alerts to fire.
The Epic Sepsis Model is the cleanest documented case of why error correction is operational labor, not a property the model ships with. The original external validation at one academic medical center found an AUROC of 0.63 with 33 percent sensitivity, far below the vendor's pre-deployment claims (Wong et al., JAMA Internal Medicine 2021). Five years later the same lead investigator validated the revised ESM v2 across four US health systems and found AUROC between 0.82 and 0.92, but with high institutional variability, positive predictive value of 0.13 to 0.26 at a 60 percent sensitivity threshold, and a number-needed-to-evaluate of 21 to 35 over a twelve-hour window (Wong et al., JAMA Network Open 2026). The model improved. The deployment problem did not. Local calibration on this population, this floor, this season is only knowable through standing local evaluation, which is operational error-correction work the deploying site has to do — exactly the maintenance layer this defense argues clinical AI requires.
Why the product is not "generate diagnosis"
The dominant framing of clinical AI in the last two years has been answer generation. The ambient scribe generates a note. The In Basket draft generates a reply. The differential copilot generates a list. Each one is positioned as helping the clinician by producing output the clinician would otherwise produce themselves. Scaling those generators does not close the gap — the training and evaluation regimes that produce capable models also reward confident guessing over calibrated uncertainty, which means more capability can produce more confident wrongness rather than less (Kalai et al., 2025).
The defense architecture argues for a different product category. The system that produces the differential is solving the wrong problem. The differential is downstream of the belief state, which is what the clinician is actually reasoning over. The system that helps is the one that maintains the structured belief state across the team, makes it inspectable when divergence matters, and runs error correction continuously against the structural failures Part 8 named.
This is the company thesis the series has been building toward, stated plainly: clinical AI is a belief-state coordination layer, not an answer layer. The answer-layer products of the last two years are useful tools (they save time, they reduce documentation burden, they catch obvious omissions); they are not the product clinical AI ultimately becomes.
How the two defenses fit together
Shared compression and error correction are complementary, not redundant. Shared compression makes the team's communication efficient when it works. Error correction catches the cases where it does not work, before the failure becomes consequential. A clinical AI that implements only shared compression produces a smoother experience that still fails silently when the codec drifts. A clinical AI that implements only error correction surfaces divergences endlessly because nothing is keeping the team's compressions aligned in the first place.
The two are also temporally distinct, which Part 10 expands. Shared compression is mostly pre-event work: training, alignment, standardization installed before the shift starts. Error correction is mostly runtime work: detecting divergence as it happens, surfacing it at the action-changing moments, repairing it before the next decision commits. Both have a post-event component: outcomes update the shared compression (training improves), and outcomes update the error-correction system (calibration improves).
The companion essays already in the series cover specific instances of error correction. The Connection names the verification architecture (signal meets explicit state across four channels). Quiet Verification covers passive-default verification with active read-back at action-changing slots. Quiet Acquisition covers the symmetric problem on the acquisition side. Each is an instance of the master architecture this essay names.
At the bedside
The cardiology fellow and the night hospitalist did the twenty-three-word handoff and the patient was safe overnight. The shared compression carried the communication. Error correction was implicit in the hospitalist's one clarifying question and would have been more explicit if the trajectory had deviated from what was expected. The system that helps tomorrow's handoff is the one that does both jobs: keeps the team's structured belief states in the same shape, and catches the cases where, despite that, the actual reasoning has drifted apart. The help is coordinating the belief state behind the handoff, not generating the handoff text.
The next move generalizes this defense across time. That is Part 10.
Compressed Medicine · Preface · 1. The Compression Substrate · 2. The Function of the Message · 3. The Highest Accurate Abstraction · 4. The Decompression Order · 5. The Minimum Sufficient Message · 6. The Grounding Constraint · 7. The Belief-State Object · 8. The Same Wall · 9. The Defense Architecture · 10. The Temporal Loop · 10.1 The Connection · 10.2 Quiet Verification · 10.3 Quiet Acquisition · 11. The Irreversible-Action Check